Lower limb alignment

Lower limb alignment
Growth and alignment vary amongst children and adults.

Parent’s will often question why their child’s feet turn in or why they have knocked knees. Most of the time, this is just a ‘normal’ alignment variation, which corrects as the child grows. However, in a small amount of cases, often the child or adult may be adopting these variations as a compensation strategy to hide a more serious issue. It is therefore important to seek medical or physio advice and have you or your child assessed correctly.
Some basic alignment variations we often see at the clinic:
In-toeing GAIT An in-toing GAIT is a postural variation where the feet are turned inwards, some even so far, that tripping over the feet occurs.
A person may turn their feet in because of the following:
1. Femoral anteversion (twisting in of the thigh bone)
Peak femoral anteversion occurs during ages 3-7, and as the child ages, the degree of anteversion normally reduces, until about 16 years of age
The degree of anteversion can progress due to habitual sleeping, sitting (e.g ‘W’ sitting) and standing postures as well as an increase in an internal torsional load applied to the growth plate (e.g walking, standing and/or running with hip, knees and feet rotating inwards)
Children who have excessive anteversion (inward rotation) are at risk of developing hip dysplasia (partial or complete dislocation of the hip). However, in some cases, children may turn their feet more in to ensure the ball of their hip sits securely in its socket.

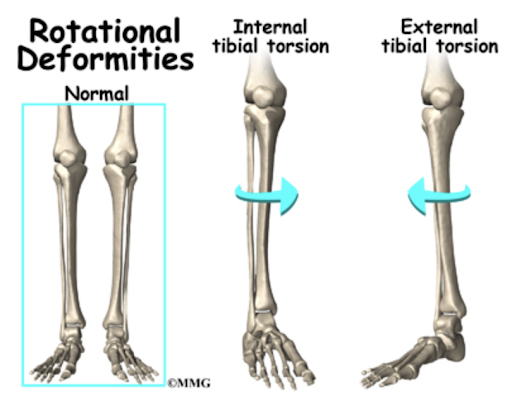
2. Internal tibial torsion (shin bone is rotated inwards)
Some children are born this way, however as they age this reduces and the shin bone starts to rotate more and more outwards (external rotation)
3. Metatarsus adductus (curvature of the foot inwards)
This normally occurs due to the babies position in the womb and may require a cast to help straighten the feet if stiff enough. Normally babies also grow out of this.
Out-toeing GAIT
An out-toing GAIT is a postural variation where the feet are turned outwards. An out-toeing GAIT normally spontaneously resolves in children. An out-toeing GAIT, is much less common and less of an issue than an in-toeing GAIT.

Femoral retroversion (twisting out of the thigh bone.
Femoral retroversion can restrict movements that require appreciable hip internal rotation, such as deep squats, patterns of full hip extension (EG/ lunging)
If you might think this is you, try turning your feet out and having a wider stance to gain depth in your squat.
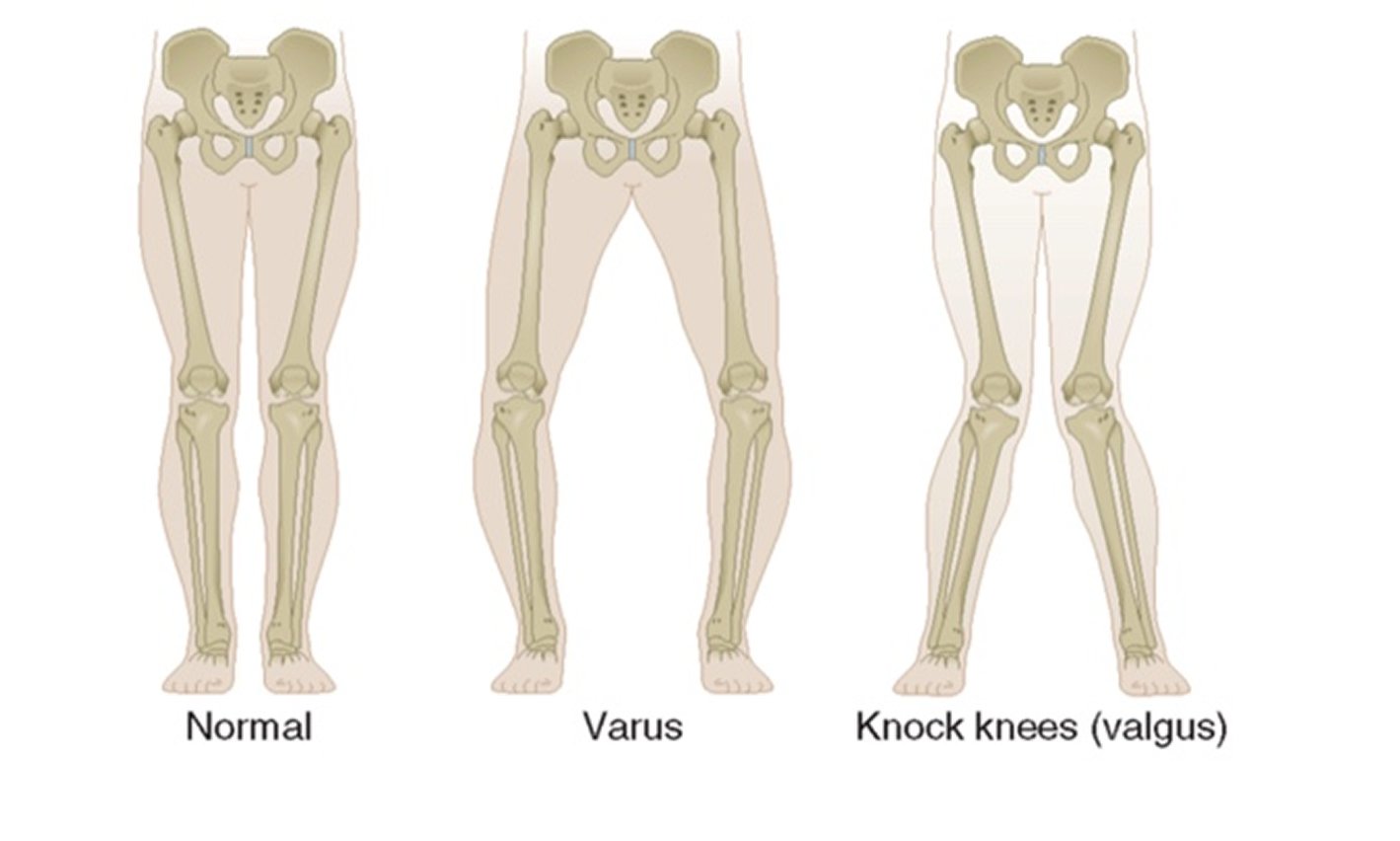
Bow legs (varus deformity).
Where the thigh bone rotates outwards and the shin bone rotates inwards causing compression on the medial (inside) aspect of the knee. People who have this appearance are unable to touch their knees when their feet are together.
We also consider this type of deformity when adults present with
Pain on the inside of their knee
Arthritis (particularly of the medial compartment)
Degenerative meniscal tears (particularly of the medial side)
Pain in the lower limb

Knocked knees (valgus deformity)
Where the thigh bone rotates inwards and the shin bone rotates outwards causing compression on the lateral (outside) aspect of the knee. People who have this appearance are unable to touch their ankles when their knees are together.
We also consider this type of deformity when adults present with
Pain on the outside of their knee
Arthritis (particularly of the lateral compartment)
Degenerative meniscal tears (particularly of the lateral side)
Pain in the lower limb